Scheduling
Guidelines:
·
First Ask
- Why is the MRCP being
requested?________________
- What prior imaging has been done (CT,
Ultrasound or ERCP)?_____________________
If prior imaging not at Cornell, please ask for copy of report and ask
patient to bring in films if possible.
- Have you had prior surgery on your
Gallbladder, Pancreas, Liver, Stomach or Intestines?_____________
What operation?__________________
- Have you ever had cancer?_____________
When was cancer diagnosed?________ What type of cancer?__________
- Do you have hepatitis or
cirrhosis?_____________
- What is the Total Bilirubin_________
·
 Schedule for 30 minutes slot in AM , preferably before 11am
Schedule for 30 minutes slot in AM , preferably before 11am
·
Patient must be
npo after midnight, may drink water only prior to MRI. This is important for making sure the
gallbladder is distended.
Patient Preparation:
· Oxygen, 2-4 liters/min by nasal canulae is useful if patient is short of breath
· Valium (5-10mg po) or Xanax (1-2 mg po) if patient is claustrophobic
Coil: Torso array, rotate 90 degrees to help eliminate wrap-around artifact.
Patient Positioning: Supine, feet first, arms crossed on chest with hands on shoulders in order to prevent arm wrap-around artifact.
Landmark: Just below xyphoid at rib cage margin.
Series
1: Locator
SSFSE shows the abdominal anatomy well. It is done preferably with a breathhold in expiration so it can be used for planning Series 2 and 3 Axial T2 and T1. It can also be performed without breath holding. Alternatively, a breath hold FMPSPGR or coronal T1 spin echo (with respiratory compensation) sequences are also adequate. With SSFSE or FMPSPGR, use a sufficiently large FOV (ie. set FOV to width of patient) to eliminate wrap-around artifact.
 Series 2: Axial T2
Series 2: Axial T2
This sequence identifies hepatic, pancreatic and other lesions. It shows the common bile duct to guide acquisition of coronal oblique MRCP sequences. If the respiratory waveform shows the pattern is breathing at regular intervals àuse respiratory triggering. If the breathing pattern is not regular then use fat saturation and 3-4 NEX. Adjust slice thickness as necessary to cover liver and pancreas in 19-20 slice so the sequence will fit on a single sheet of film.
Series 3: Axial in-phase (fat saturation)
This sequence is excellent for evaluating pancreatic pathology and especially for identifying pancreatic masses. Cover the entire pancreas. If necessary, the slice can be made thicker if more coverage is needed. It must be performed with breath holding. If the patient can not suspend breathing long enough, consider T1 spin echo (6 mm thick slice interleaved) with fat saturation.
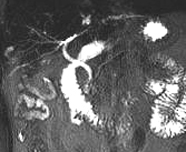 Series 4: MRCP (Thin Slice)
Series 4: MRCP (Thin Slice)
The purpose of this sequence is to comprehensively image the biliary system in patients suspected of biliary obstruction, stones or post liver transplantaion. It may be acceptable to perform just on straight coronal acquisition. But a more comprehensive study includes both oblique acquisitions.
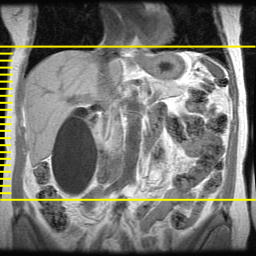
· Prescribe this series from the axial T2 series. Select an image which shows the common bile duct (CBD).
· Use 5 mm thick with 0 gap slices
· 15 slices takes about 30 seconds, which is reasonable breath hold. Although breath holding is not essential, it does make reformations possible
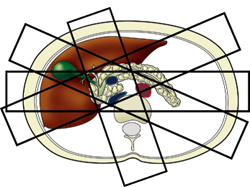
Coronal View: Set the imaging volume from posterior to the CBD as it passes through the head of the pancreas to anterior to the parta hepatis. Ideally the entire gallbladder should be included within the 15 slices, but if it extends too far anteriorly, you may have to exclude part of the gallbladder in order to image the entire CBD.
RAO: Rotate 20-30 counterclockwise and include the CBD. Do not worry about excluding part of gallbladder.
LAO: Rotate 20-30 clockwise centered on the CBD and be sure to include entire gallbladder.
Axial: Set the axial plane at 4-5 mm slice thickness is useful in patients with suspected of pancreatic divisum.
|
|
|
|



Series
5: MRCP (Thick Slib)
This alternative approach to MRCP acquires an image of the entire biliary system in just 2 seconds. Use oblique prescription and hold shift key down to prescribe multiple slabs at different angles.
Filming
Instructions:
Film each series on 1 sheet of film.
Billing
Instructions:
ICD9
Codes:
Choledocholithiasis: 574.5
Cholelithiasis: 574.9
Bile duct obstruction: 576.2
Sample
Normal Dictation:
Technique: - Coronal SSFSE
- Axial T2 with respiratory triggering
- Axial T1 weighted spoiled gradient echo, in-phase with fat saturation of pancreas
- Coronal oblique RAO & LAO thin slice and thick slab MRCP
There is no dilation of the intra or extra-hepatic bill ducts. The gallbladder is normal; no gallstone identified. The pancreas has a normal T1 bright appearance; no pancreatic mass identified. There is no dilation of the pancreatic duct. The liver, spleen, adrenal glands and kidneys are unremarkable, no adenopathy is identified.
Impression: Normal MRCP, no biliary or pancreatic duct obstruction.